In the upper part the body of the humerus is rounded, and closer to the distal epiphysis it is triangular. On the body there are: posterior surface (lat. facies posterior), limited by the lateral and medial edges (lat. margo lateralis et medialis); medial anterior surface (lat. facies anterior medialis) and lateral anterior surface (lat. facies anterior lateralis), which are separated by an inconspicuous ridge.
The proximal epiphysis is represented by the head of the humerus (lat. caput humeri), separated from the diaphysis by an anatomical neck (lat. collum anatomicum). The head articulates with the glenoid cavity of the scapula, forming the shoulder joint. Behind the neck there are two tubercles (apophysis) - the larger and the smaller (lat. tuberculum majus et minus), between which runs the intertubercular groove - the site of the tendon of the long head of the biceps brachii muscle. Below the tubercles, at the border with the diaphysis, there is a surgical neck (lat. collum chirurgicum) - the site of the most common fractures of the humerus.
On the body of the bone there is a deltoid tuberosity (lat. tuberositas deltoidea), to which the deltoid muscle is attached. Posterior to the tuberosity, a groove runs in a spiral from the medial to the lateral side radial nerve(lat. sulcus nerve radialis) .
On the distal epiphysis there is a condyle (lat. condylus humeri) and on the sides of it there are two epicondyles - medial and lateral (lat. epicondylus medialis et lateralis ). Between the epicondyles there is a surface for articulation with the bones of the forearm, divided into a block of the humerus (lat. trochlea humeri) and the head of the condyle of the humerus (lat. capitulum humeri). Above them on the front side, respectively, are the coronal (lat. fossa coronoidea) and radial (lat. fossa radialis) fossa, as well as behind the ulnar fossa (fossa of olecranon, lat. fossa olecrani), which are necessary for articulation with the ulna and radius bones, forming the elbow joint. On the posterior side of the medial epicondyle there is a groove for the ulnar nerve (lat. sulcus nerviulnaris) .
Ossification
At birth, only the proximal epiphysis consists of cartilage tissue, due to which the head of the humerus is practically not visible on the x-ray. During maturation, three points of ossification of the proximal epiphysis successively appear:
- In the medial part of the head of the humerus (0-1 year or from birth);
- In the greater tubercle and in the lateral part of the head (2-3 years);
- In the lesser tubercle (3-4 years);
By 4-6 years, these centers merge into a single head of the humerus. Replacement of metaepiphyseal cartilage at the border of the proximal epiphysis and diaphysis with bone tissue (synostosis) occurs in adolescence, due to which the bone continues to grow in length. An x-ray of a child or teenager reveals a characteristic light area at the site of the metaepiphyseal cartilage, which can be mistaken for a fracture or fissure.
Humerus(humerus; Fig. 18). This is a long tubular bone, has a body - the diaphysis and two ends - the epiphyses. The upper (proximal) epiphysis is a spherical formation - this is the head of the humerus, through which the humerus articulates with the glenoid cavity of the scapula, forming the shoulder joint. The head is separated from the rest of the bone by a narrow interception - the anatomical neck. Behind the anatomical neck there are two tubercles: the small tubercle is directed anteriorly, and the large tubercle is oriented to the lateral side. Between the tubercles lies the intertubercular groove. Muscles are attached to the tubercles, and the tendon of the long head of the biceps brachii muscle passes through the groove. Below the tubercles, a wide, gentle narrowing is visible - the surgical neck, so named because fractures of the humerus are more often observed in this place.
The body of the humerus in the upper parts is cylindrical in shape, and downwards it becomes triangular. Above the middle of the body of the humerus, on the lateral side, a roughness called the deltoid tuberosity is noticeable, the place of attachment of the muscle of the same name. Around the body, from top to bottom, first along the medial, then along the posterior and lateral sides, a wide, gentle spiral groove descends - the groove of the radial nerve.
The lower (distal) epiphysis of the humerus is wide, flattened in the anteroposterior direction. Its medial articular surface of a cylindrical shape - the block of the humerus - serves for articulation with the ulna. Above the trochlea, on the anterior surface of the humerus there is the coronoid fossa, and on the posterior surface there is the olecranon fossa. The lateral articular surface - the head of the condyle of the humerus - is spherical, articulates with the articular surface of the head of the radius. Above the head of the condyle of the humerus is the radial fossa. On both edges of the lower epiphysis, above the articular surfaces, are the medial and lateral epicondyles. They serve to attach the muscles of the forearm.
Bones of the forearm. The ulna (ulna) and radius (radius) bones are long, tubular, triangular (Fig. 19). Their upper (proximal) and lower (distal) epiphyses are in contact, and the diaphyses are curved in opposite directions in such a way that the interosseous space of the forearm is formed between them.
![]()
The upper (proximal) epiphysis of the ulna is massive, bears a trochlear notch, covered articular cartilage. The notch is bounded above by the olecranon process, and below by the coronoid. On the lateral side, on the proximal epiphysis there is a radial notch with an articular surface for articulation with the head of the radius. The ulnar tuberosity is visible on the anterior surface below the coronoid process.
The distal epiphysis is represented by a head with an articular circle for articulation with the radius. In the posteromedial region, the distal epiphysis ends with the styloid process of the ulna.
The proximal epiphysis of the radius is narrow, represented by a head with an articular circumference. Below the epiphysis, the neck of the radius is clearly visible, and below it is a protruding tuberosity for the attachment of the biceps brachii muscle. The diaphysis of the radius, like the ulna, is triangular and passes into a massive distal epiphysis, from the lateral side of which the styloid process extends. On the medial side, on the distal epiphysis there is an ulnar notch with an articular surface for articulation with the ulna. The lower surface of the distal epiphysis of the radius articulates with the bones of the wrist.
Bones of the hand. The bones of the hand are divided into the bones of the wrist, metacarpus and finger bones (phalanx) (Fig. 20).
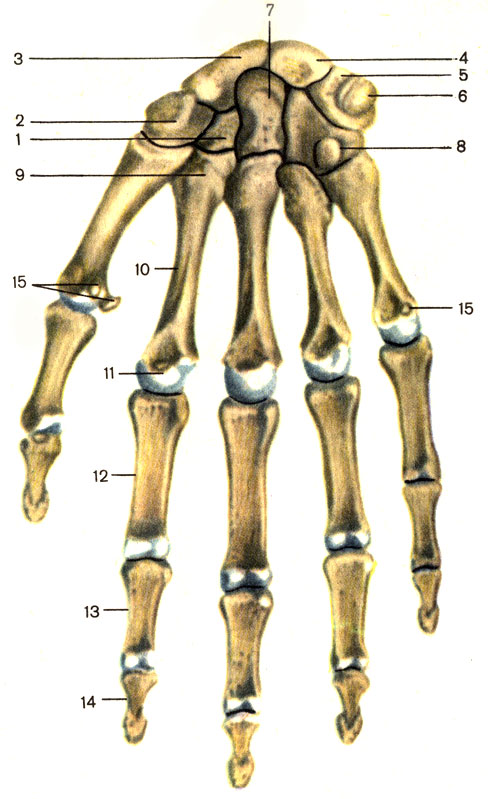
The carpal bones (ossa carpi) are short, irregular in shape, arranged in two rows. The proximal row consists of the scaphoid, lunate, triquetrum and pisiform bones, and the distal row consists of the trapezoid, trapezoid, capitate and hamate bones. All the bones of the wrist lie in the same plane, but this plane is curved in the form of a groove: concave on the palmar side, and convex on the back. The three bones of the proximal row: the scaphoid, lunate and triquetrum - form an elliptical convexity that articulates with the distal epiphysis of the radius. All the bones of the distal row of the wrist are connected by a broken line of joints to the metacarpal bones.
The bones of the metacarpus (ossa metacarpi) are tubular, have a base, a body and a head. Their bases are connected to the distal row of carpal bones, and their head is connected to the bases of the phalanges. The metacarpal bones are curved along their length: their concavity faces the palmar side of the hand, and their convexity faces the back. The first (I) metacarpal bone is the shortest and widest, and the II is the longest.
Phalanges. The skeleton of the first finger has two phalanges, and the rest have three. There are proximal, middle and distal phalanges, and each phalanx has a body, base and head.
Bones shoulder girdle is a strong foundation for numerous muscles, tendons and ligaments. It's no secret that the top and lower limb- This is human movement, the ability to perform various types of work. In order for the hands to be most developed and functional, a sufficiently solid bone base and strong joints are needed.
Nature has provided for everything in man, so the upper one consists of the scapula, collarbone, humerus, ulna and radius bones, as well as small bones of the hand. Accordingly, muscles are attached to all these bone bases, thanks to which the hand is able to carry out movements.
The humerus is one of the largest and most massive bones in the human body. It consists of a diaphysis, or the tubular body of the bone, and two epiphyses, which are the articular surfaces.
If you take a closer look at the anatomy of this formation, you will notice how functionally thought out this bone is.
Like any surface, the humerus has a weak point - the surgical neck; this is where the bone most often breaks. However, the muscular frame is designed in such a way that when physical activity it is in this place that it grows most intensively muscle mass, thereby protecting the bone.
In addition, the humerus has several projections, or tubercles, to which the largest muscles of the shoulder are attached. Ridges or elevations extend from the protrusions, between which the intertubercular groove is located - this is where the tendon attaches
In the area of the lower epiphysis there are two condyles, and above them two epicondyles - these are also peculiar bone tubercles, which are part of this. There are also two fossae - the ulnar and coronoid, they are necessary for a more dense comparison of the processes of the ulna and radius.
The humerus is a rather complex structure, and in addition to its supporting function, it also performs a number of others. For example, hematopoietic. As you know, everyone is an organ that produces red blood cells. In the spongy substance of the bone is located which performs this function.
In addition, spongy bone is capable of producing factors that affect the immune system and blood clotting.
It should be noted that the size and diameter of the bone is individual for each person. It depends on the growth, number of applicants nutrients and from hereditary predisposition. Often we have to deal with a situation where patients have increased fragility or brittleness of bones due to a deficiency of calcium and other microelements. This process can be formed in utero.
Shoulder fractures are common in early school-aged children and the elderly. This is due to the lifestyle of the former and a decrease in physiological strength in the latter case.
During a fracture, the humerus is destroyed at its weakest point - in the area of the surgical neck, but there are other types of fractures. In children - a subperiosteal fracture of the “green stick” type, and in adults, fractures with displacement of fragments.
In any of these situations, the patient needs qualified help.
Osteosynthesis of the humerus can be performed in several ways. There is a special one that allows you to fasten existing fragments. The insertion of wires can be carried out at absolutely any level and near the joints. The difficulty is in inserting the needles in the area of the upper third of the shoulder on the inner surface (in the axillary region), because this brings discomfort and inconvenience to the patient, so in this area the needles are inserted in an X-shape.
In order to most correctly align the fragments, you can use the skeletal traction method before installing the apparatus.
Traumatologists often use special plates and screws for osteosynthesis of the humerus if the area of damage is not too large and the number of fragments does not exceed 3-4 pieces.
Table of contents of the topic "Shoulder joint (articulatio humeri). Anterior region of the shoulder.":1. Shoulder joint (articulatio humeri). External landmarks of the shoulder joint. Projection of the joint space of the shoulder joint.
3. Fibrous layer of the joint capsule. Ligaments of the shoulder joint. Muscles that strengthen the shoulder joint.
4. Synovial bursae of the shoulder joint. Topography of the synovial bursae of the shoulder joint. Ways of spread of purulent processes in the shoulder joint.
5. Collateral circulation in the area of the shoulder girdle. Scapular arterial collateral circle. Occlusion of the axillary artery. Impaired blood flow in the axillary artery.
6. Anterior shoulder area. External landmarks of the anterior shoulder area. Boundaries of the anterior region of the shoulder. Projection onto the skin of the main neurovascular formations of the anterior region of the shoulder.
7. Layers of the anterior region of the shoulder. Anterior fascial bed of the shoulder. Muscle Casserib. Posterior fascial bed of the shoulder. Walls of the fascial bed of the shoulder.
8. Topography of vessels and nerves of the anterior fascial bed of the shoulder. Location of nerves and blood vessels on the shoulder.
9. Connection of the fiber of the anterior region of the shoulder with neighboring areas. Holes in the anterior region of the shoulder. Messages from the anterior shoulder area.
Humerus has a spherical shape at the top articular head, which is separated from the rest of the bone by a narrow groove called anatomical neck. Immediately behind it there are two muscle tubercles, of which the larger one, tuberculum majus, lies laterally, and the other, smaller one, tuberculum minus, lies slightly anterior to it. Between the tubercles there is a groove, sulcus intertubercularis, in which the tendon of the long head of the biceps brachii muscle passes. Directly below both tubercles, at the border with the diaphysis, is located surgical neck of the humerus.
In the shoulder joint there is a large discrepancy between the almost flat articular end of the scapula and the ball-shaped head humerus. This discrepancy is to some extent smoothed out by the cartilaginous articular lip, labrum glenoidale, which increases the volume of the cavity without limiting mobility, and also softens shocks and shocks when the head moves. However, the remaining incongruity is the cause of humeral dislocations, which occur more often than in any other joint.
Rice. 3.12. Shoulder joint in longitudinal section (according to Spalteholz, with modifications). 1 - lig. transversum scapulae; 2 - processus coracoideus; 3 - capsula articularis; 4 - tendo m. bicipitis brachii (caput longum); 5 - vagina mucosum intertubercularis; 6 - humerus; 7 - recessus axillaris; 8 - labrum glenoidale; 9 - scapula; 10 - spina scapulae.Joint capsule shoulder joint loose and relatively thin. It is attached on the scapula to the bony edge of the glenoid cavity and, covering the head of the humerus, ends at the anatomical neck. In this case, both tubercles remain outside the joint cavity. From the inside and below, the articular capsule is attached much lower, at the level of the surgical neck of the shoulder, forming the so-called axillary inversion, recessus axillaris (Fig. 3.12).